


"The difficult lies to detect are lies our minds wish they were true." -Aniekee Tochukwu Ezekiel
Articles from the Vaccine Wars can be found here. See Part 1, Part 2, and Part 3 if you're just getting started. This may be necessary to handle all the acronyms, and if you're truly interested in unraveling the vaccine effectiveness illusion, this is the article you're going to want to read carefully and understand.
All the green lines are straight. The illusion is in the periphery.
For the sake of this article, I would like readers to keep multiple points in mind:
HUB = WUB = EUB (health is wealth is education, as variables, in aggregate)
It may very well be that HUB accounts for all of VE in U.S. county level data, but may be a small or moderately-size part of the illusion in other nations.
If VE is effectively zero in any one nation, then there is likely no complete mechanism for effects of these biological products at all, so any VE in any data set is an illusion. I focus my primary data argument on the U.S. county data via the CDC.
While I led this article series with a graph that showed that the slightly negative correlation between vaccine uptake and COVID-19 deaths basically tracked (was slightly higher than, on average) median household income by U.S. county, that is not alone enough to declare that the HUB validates the ZEH. It would be irresponsible to stop there and scream from the hills, "These quasi-vaccine genetic products don't stop COVID!" So, I've gathered further evidence. A lot of it. Understand that the graphs in this article are a fraction of those that I have available, and may include in a more complete book on the topic. Walk with me…
I'm going to lead with the punchline again. All correlation between vaccine uptake and COVID-19 mortality rates by county appears to be completely explained by income and education status. The correlations are almost perfect mirror images of one another!
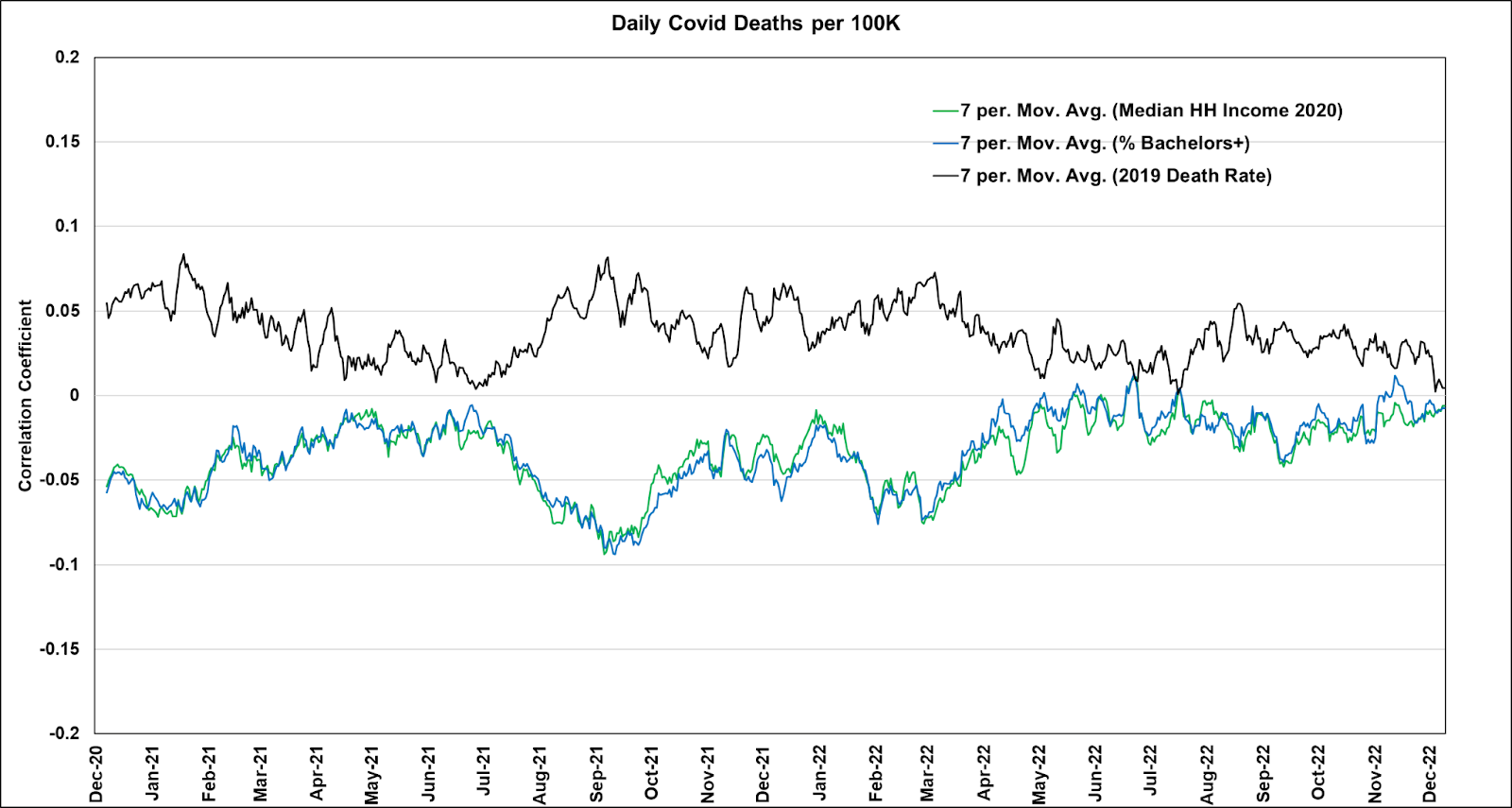
This chart screams HUB and ZEH, but let's look for other evidence..
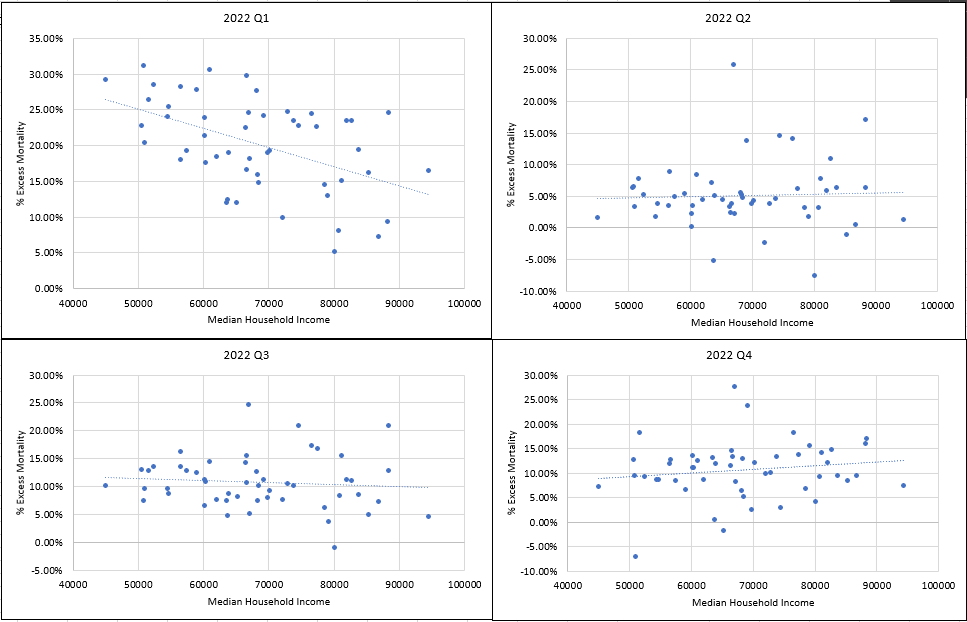
Consider these two charts I made last year of all cause mortality (per million residents) for all U.S. counties where the x-axis represents the percentile score for median household income (a good proxy for wealth).
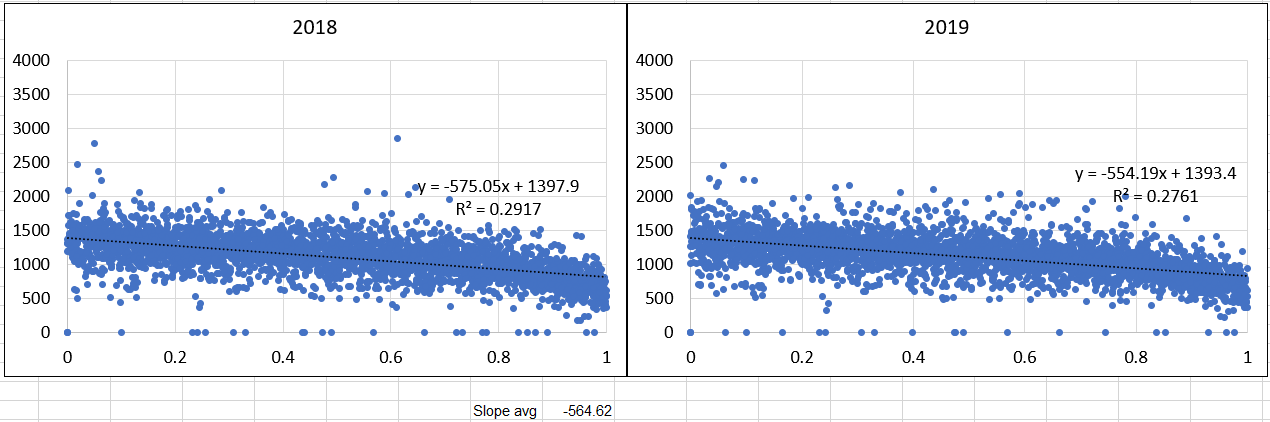
Clearly, poorer counties suffer substantially higher mortality rates (almost 68% higher from the lowest income to the highest earning counties). Clearly, these are not equivalent cohorts, and any analysis that clumsily mashes them together will necessarily suffer from the ecological fallacy in a way that drives up VE. But this is not my point for the moment.
Now, look at the same charts for 2020 and 2021. The slopes of the trendlines tilt a little more, meaning that the mortality increase among poorer counties was significantly higher throughout the pandemic—both before and after the vaccines were rolled out.
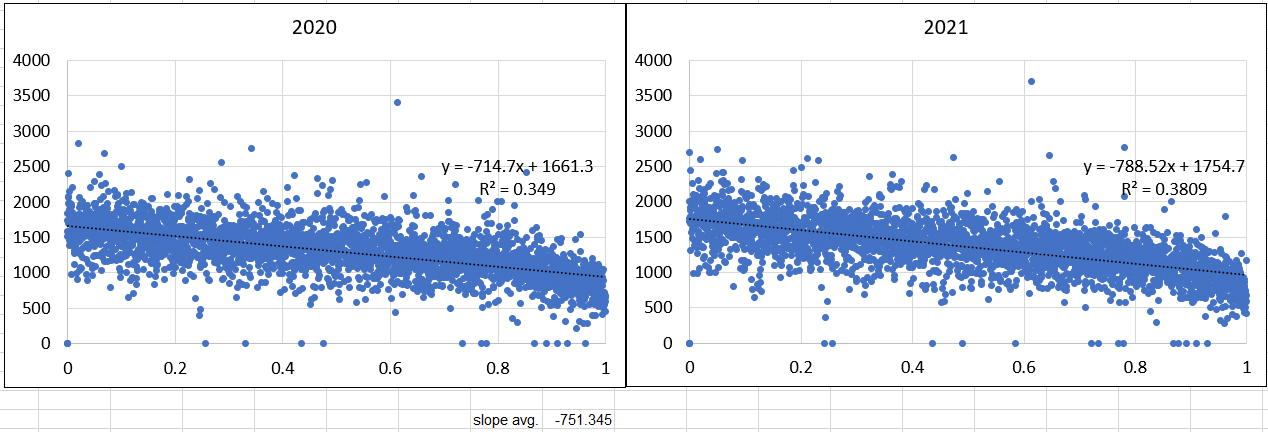
The slope got sharper during COVID, so apparently COVID kills the poor faster. COVID mortality was a bit higher in 2021 than in 2020, and the slope tilted just a bit more negative. If the vaccines were effective, we should see a sharper change—the tilt toward the wealthier counties should be more extreme. In fact, if we combine the 2021 and 2022 slopes through May 22, 2022, we get -646.33, which is a softer slope than in 2020 before the vaccines rolled out, which is the exact opposite of what we would see if the vaccines were effective at reducing death.
Of course, this is all cause mortality, which means that other variables affect the slope. These include changes in rates of obesity and diabetes that make COVID-19 a more severe disease, murder and suicide rates, and drug overdoses. The problem is that these all affect poor counties more severely, which would have the effect of making the slope sharper, so a softer slope post-vaccine than before looks extremely bad for the hypothesis that the vaccines are effective.
Now, I do have the state-level data ready through all of 2022, and while the advantage in excess deaths began the year tilting toward the wealthier, more vaccinated states, that trend began to reverse in 2022. The crowd that argues "waning efficacy" should only see a partial flattening of the trend, but not a reversal.
Over at I Numero, T Coddington has been performing a parallel self-education similar to my own. He graphed serious indicators of poor health versus booster uptake showing much great dose administration in areas where the people are healthier.
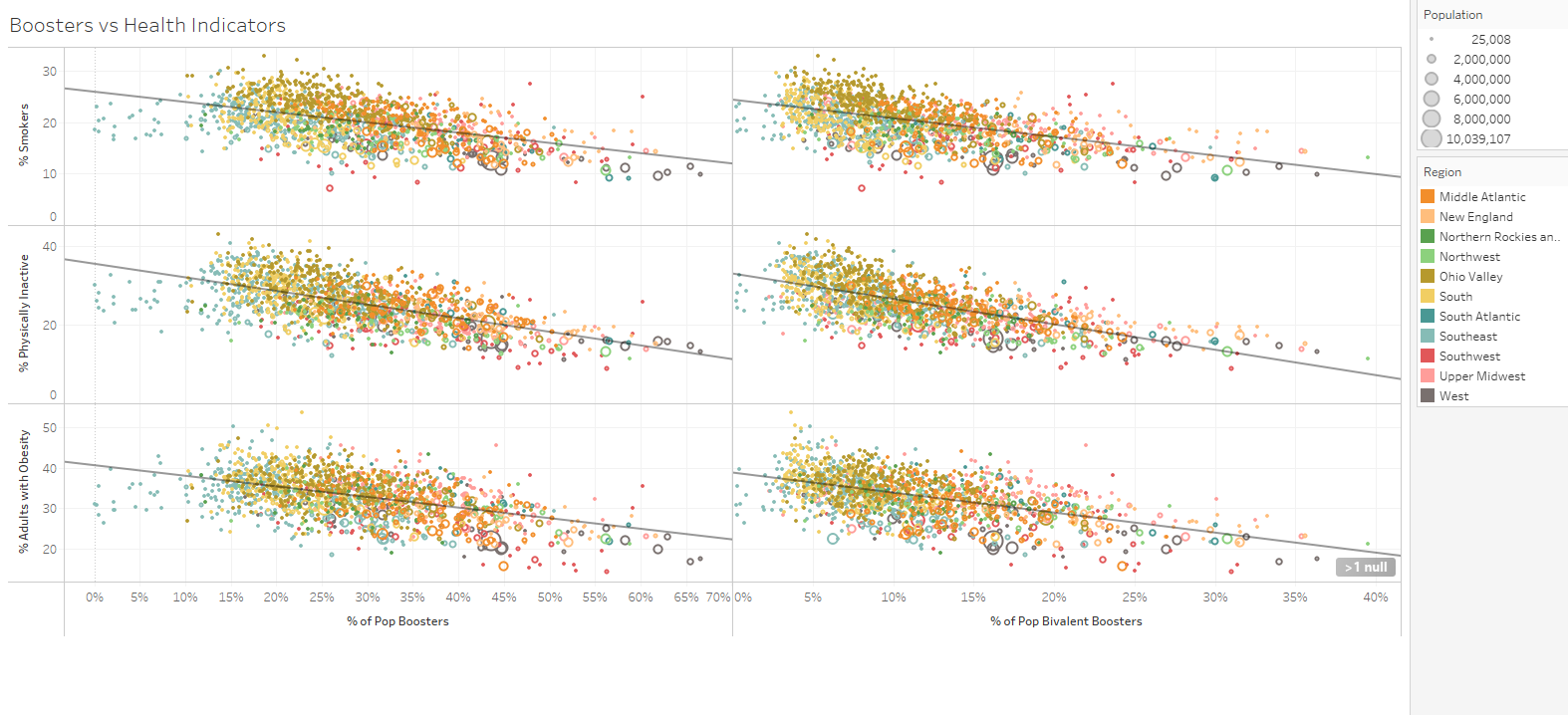
Hat tip: T Coddington
There is no possible way that these graphs can be confused: healthier Americans were substantially more likely to get vaccinated. And that only makes sense given the strict mandates put in place for groups that include large numbers of the healthiest Americans: many colleges applied strict mandates, resulting in vaccination rates up to nearly 100%, thumbs were on the scales to push corporate workers into vaccination, and
More specifically, he firms up my claim that "wealth is health"!
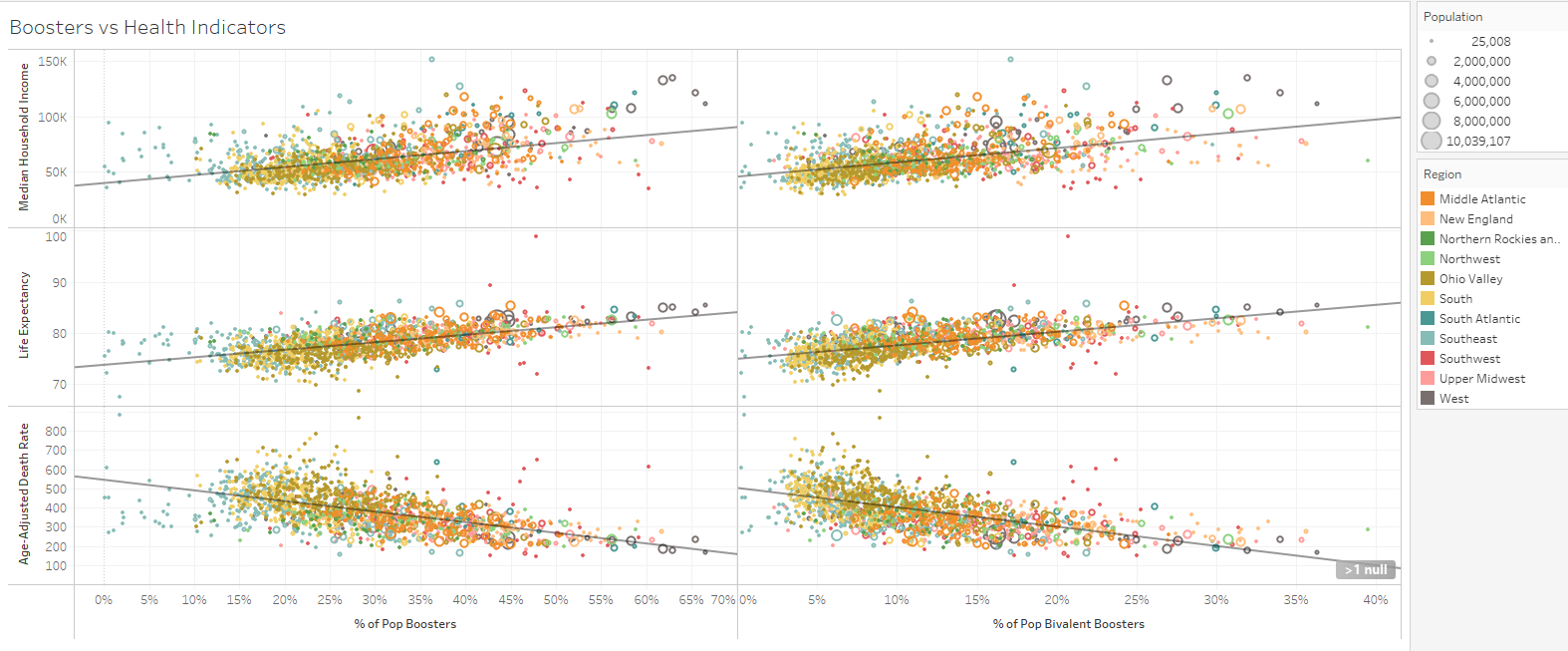
I think that T Coddington has had a similar journey to my own over the past year, recognizing key health/wealth correlates, then discovering the literature (that authorities damn well surely know about) on the HUB.
While the graphs we just saw were based on U.S. county-level aggregates, there is research (in addition to the VSD's publication) that shows the HUB on a more individual level. And that's without mandates that pushed young people (military, college students, corporate workers) into vaccination.
Here is another scatter plot with U.S. county data as of mid-August 2022 (h/t Operation Uplift), this time with both axes rank-ordered (each number is ranked from 1 to the total number of counties, in strictly increasing order). The lack of clustering is another way to see how little relationship exists between vaccination rates and COVID-19 spread.
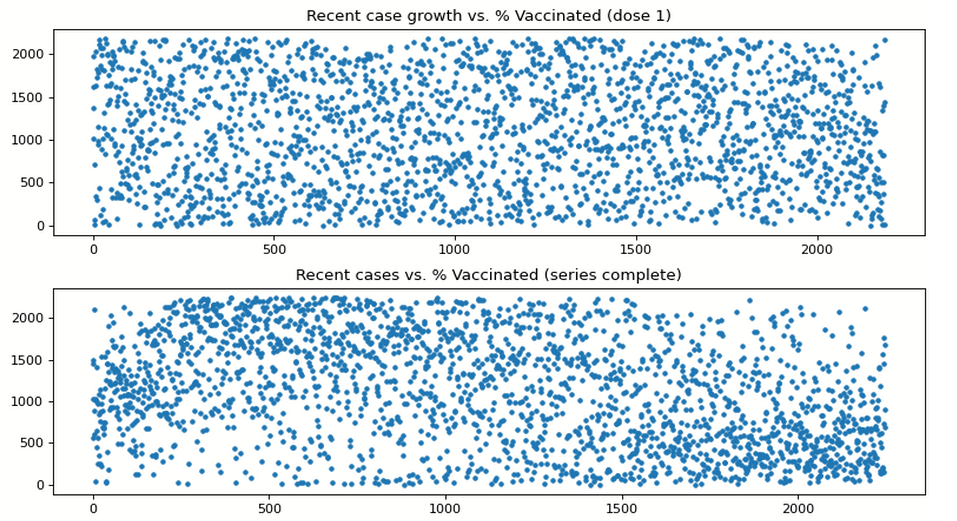
Before we talk about breakthrough cases, let's talk about R again for a moment. The following plots were provided by computer scientist Timothy Snyder, a volunteer with Operation Uplift. The scatter plots compare vaccination rates with viral spread across U.S. counties. Do you see a trend line? Overall? Or for any one color (month)? I sure don't.
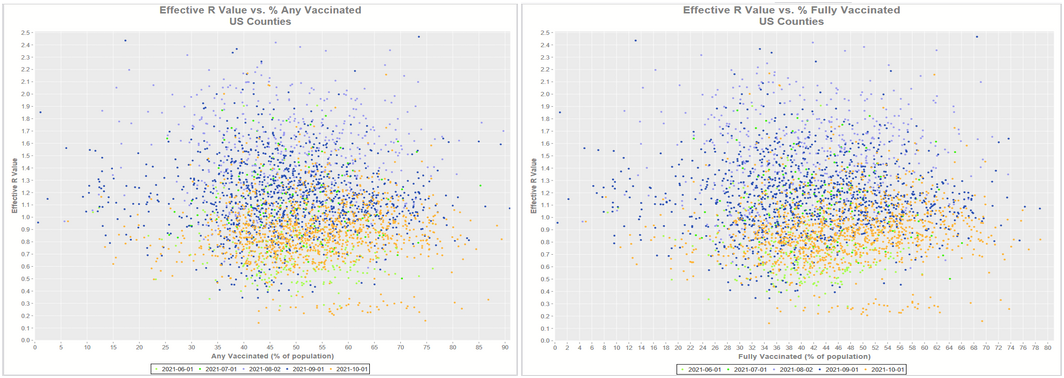
What we see in these charts is that there is no significant correlation between vaccination rates and spread---at least by some definition, which we'll put a pin in and come back to later. But this is at least interesting on its own because it presents a puzzle where "efficacy" (defined only as relative risk reduction) of the vaccines occurs entirely without any absolute risk reduction of the system. If there is relative risk reduction without absolute risk reduction, that means that vaccinating a cohort of individuals somehow prevents infections that take place in that cohort while pushing infections into the remaining unvaccinated cohort. That would be quite bizarre, but would also imply that the effects of the vaccine would not be a public health concern, on the whole. Either that, or somehow, in a way that would seem quite magical, only the people who were never going to get sick got vaccinated (basically), which is evidence of the HUB sculpting the relative risk reduction.
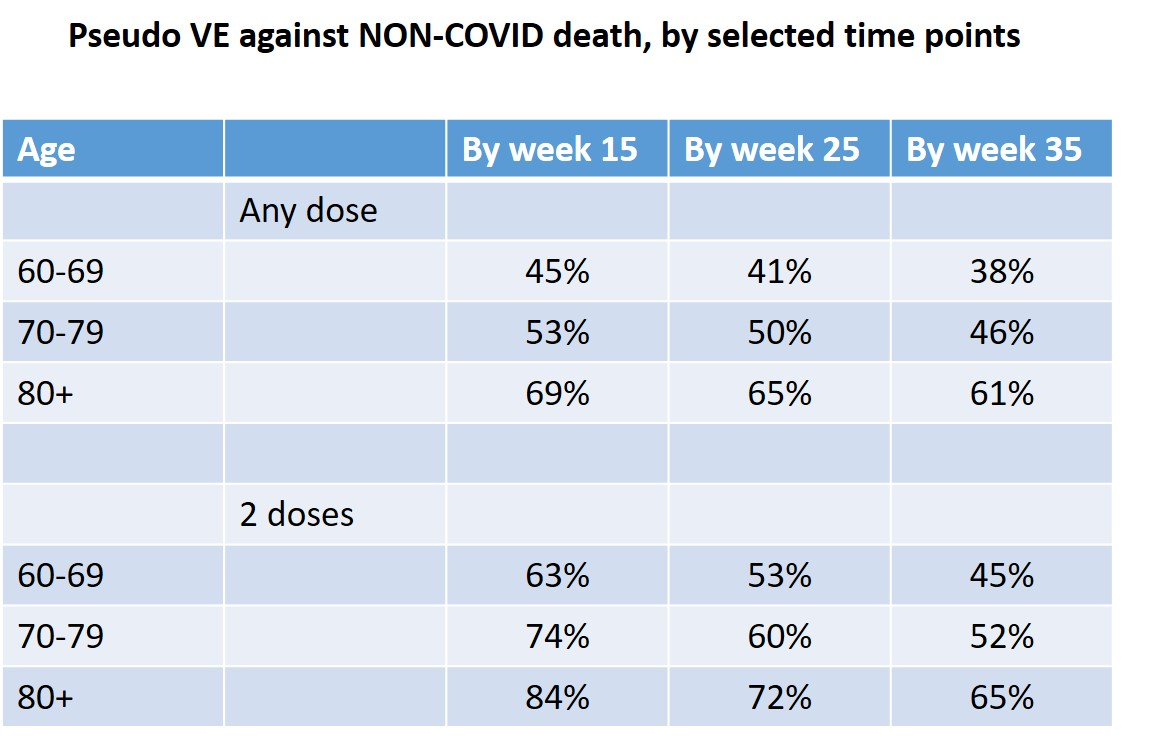
Epidemiology and Biostatistics Professor Emeritus Eyal Shahar agrees that HUB has been at play, artificially elevating VE with what he calls "pseudo-protection".
Not everyone agrees that HUB is entirely to blame for potentially false appearances of substantial VE. In a paper uploaded to researchgate last year (Neil et al, 2022; preprint), a deep team of investigators analyzed COVID-19 mortality data by vaccine status as presented by the UK's Office of National Statistics (ONS). They concluded that healthy vaccinee bias explained less of the VE than delays in reporting of vaccination status combined with systemic miscategorization of deaths.
The risk/benefit of Covid vaccines is arguably most accurately measured by comparing the all-cause mortality rate of vaccinated against unvaccinated, since it not only avoids most confounders relating to case definition but also fulfils the WHO/CDC definition of "vaccine effectiveness" for mortality. We examine two of the most recent UK ONS vaccine mortality surveillance reports, which provide the necessary information to monitor this crucial comparison over time. At first glance the ONS data suggest that, in each of the older age groups, all-cause mortality is lower in the vaccinated than the unvaccinated. This conclusion is cast into doubt upon closer inspection of the data due to a range of fundamental inconsistencies and anomalies in the data. Whatever the explanations for these are, it is clear that the data is both unreliable and misleading. It has been suggested that the anomalies are the result of healthy vaccinee selection bias and population differences. However, we show why the most likely explanations for the observed anomalies are a combination of systemic miscategorisation of deaths between the different categories of unvaccinated and vaccinated; delayed or non-reporting of vaccinations; systemic underestimation of the proportion of unvaccinated; and/or incorrect population selection for Covid deaths. We also find no evidence that socio-demographic or behavioural differences between vaccinated and unvaccinated can explain these anomalies.
Could the answer be a combination of miscategorization and HUB? Since I am more familiar with the U.S. data, I will focus there. After all, if the experimental quasi-vaccines aren't effective in one nation, it stands to reason that they aren't effective in any nations. And while we should expect VE computations [corrected for bias where necessary] to be highly similar between nations, there is no reason to expect that HUB should be the same from one nation to the next. The HUB is highly sensitive to policy decisions made qua nation. For instance, mandates focused on members of the military and universities should be expected to introduce the HUB among young adult demographics.
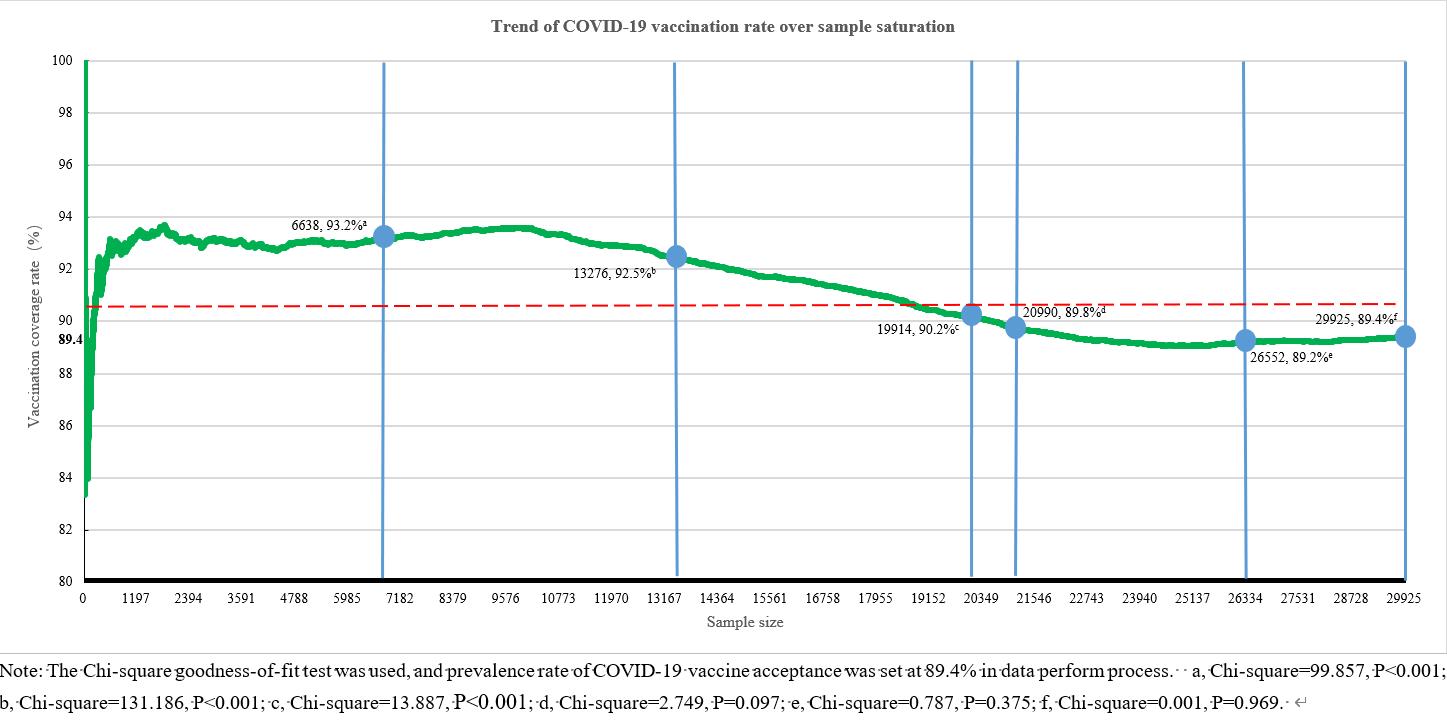
It's not just in the U.S. where HUB is clearly and substantially observed. Studies around the world tend to point toward consistently unidirectional HUB bias. A study out of China (Miao et al, 2022) examined the relationship between COVID-19 vaccine uptake and 12 different healthy lifestyle habits. In all 12 cases, there was positive correlation in all 12 cases. Since the vast majority of China (91.8% now; 89.4% in the study) is vaccinated, this pools the least healthy people into the unvaccinated category.
In a recently published study (Kwan et al, 2023), researchers found baseline rates of diabetes to be 41% lower among the vaccinated. Though this measurement did not quite achieve statistical significance, it seems clinically meaningful—particularly in light of all of the other evidence that the vaccinated are a substantially healthier cohort.
We also have the vaccine trial data itself (Benn et al, 2022; still preprint?) to demonstrate that the HUB works to massage the illusion of effectiveness into retrospective vaccine analyses. There was no overall mortality benefit whatsoever for the mRNA vaccines during their trials.
Consistency Across Observations
While there is no "proof" in science or statistics, we love to examine problems from different vectors. We gravitate toward hypotheses that are consistent with all observations.
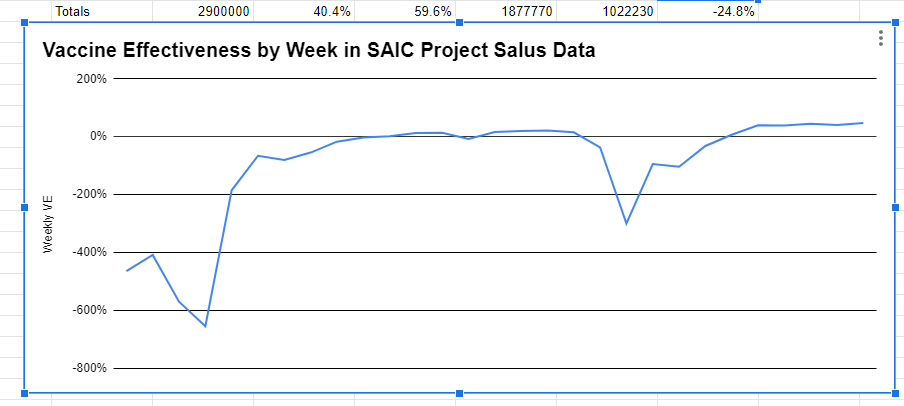
Recall now that after a basic correction over risk-adjusted person days, the quickly scrubbed data from the military contractor SAIC showed negative efficacy shortly after vaccination, which asymptotically moved toward zero efficacy thereafter.
In Japan, researchers (Aug 2022 Med Check, Vol. 8, No. 24r) discovered two cases of data manipulation by the Japanese Ministry of Health, Labor, and Welfare. Emphasis mine:
One is the case of misregistration of vaccine recipients. When comparing the proportion of newly reported COVID-19 patients by vaccination status, patients who were surely vaccinated but with unknown date of vaccination were treated as “unvaccinated” by MHLW. Hence, the proportion was extremely low in the vaccinated and extremely high in the unvaccinated. As a result, the data gave the impression that the vaccine worked very well.
The data from April 11 onwards have been corrected as pointed out by a researcher. As a result, the proportion of new infections per 100,000 people no longer differs across most age groups. Considering the “healthy vaccinee effect”, the protective effect of vaccine is even lower.
Interested readers can also read later in the article about increases in myocarditis rates among young, healthy Japanese citizens, post-transfection. But this article is primarily focused on the benefit side of the risk-benefit analysis—specifically the fact that there doesn't appear to be any.
Also, let us not forget studies showing similar viral loads between the vaccinated and unvaccinated populations (Riemersma et al, 2021). So, all those magical antibodies aren't doing their jobs, but this is supposed to slow mortality?
It didn't.
Even worse, in a reply to the concerns of Statistics and data experts Norman Fenton, Martin Neil (seen on RTE here), Clare Craig, and Scott McLachlan, the UK's Office of National Statistics (ONS) admitted that their publicly presented data summaries suffer from vaccine status errors and demographic skews that likely embeds some amount of HUB into the results (at least for some demographic bands).
…For an individual to be included in the PHDA, they must have responded to the 2011 census and be presently registered with a GP. Approximately 79% of the population fall into this category. Those missing from the PHDA dataset are therefore not missing at random, and they are more likely to fall under one or more of the following categories:
Younger in age
Born outside of the UK
Unvaccinated (as it is more difficult to obtain a COVID-19 vaccination without being registered with a GP)
We consider that it is therefore likely that the sample used in the Deaths by Vaccination Status publication is not representative of the general population. Those who are missing are, we think, more likely to be younger and unvaccinated. This is also acknowledged by ONS in its Deaths by Vaccination Status publications.
ONS is working to address some of the sampling issues present in the first six iterations of the publication…
And while the ONS data does not seem to suffer from as severe a degree of HUB skew as the U.S. county data, one of the frightening things that I discovered when I examined the publicly available ONS data set in May 2022 was that the ONS admitted at the time (as a note in their own spreadsheet) to excluding over 2,000 COVID-19 deaths from their data set—all of whom died shortly after vaccination.

Maybe some of those deaths were due to vaccination, and maybe they weren't, but it does stack the deck not to include the COVID-19 illness rates among the most frail, which is itself a form of HUB.
Globally, the wealthiest nations were generally the most highly vaccinated, though vaccine uptake in the second quartile nations was highly similar to that of the highest quartile nations.
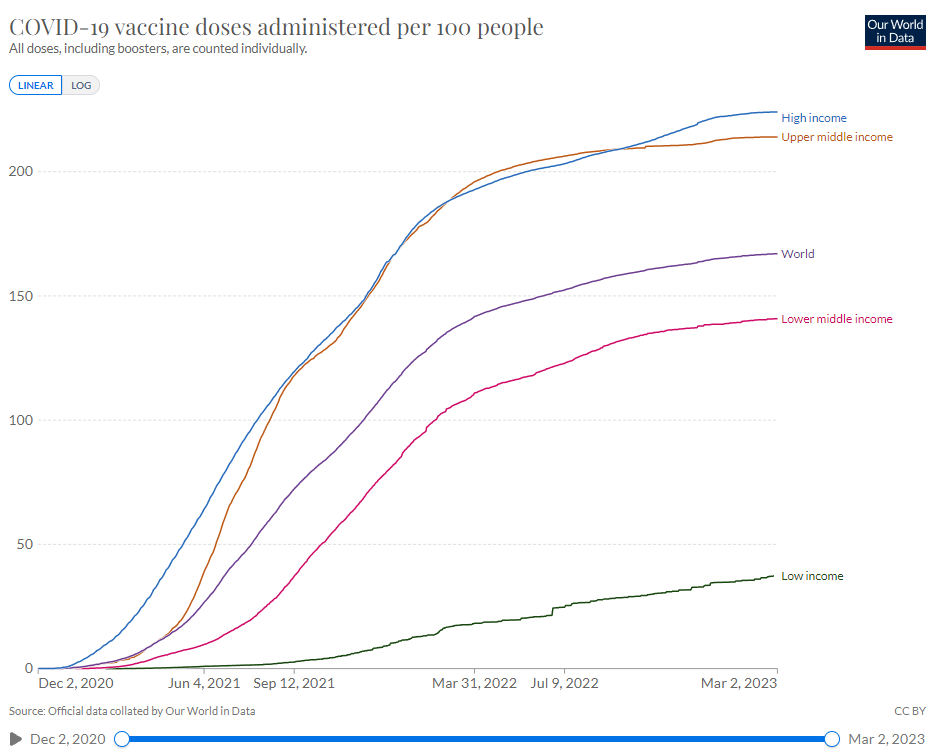
So, did those nations see similar changes in their rates of COVID-19 mortality?
No. In fact, the results look absolutely nothing alike.

If the vaccines were effective, why do we see such dramatic divergence between high income and upper middle income nations more than two years into the experimental mass vaccination program? Is it because the mRNA vaccines more often used among the wealthier nations simply don't work at all? It would seem that way, but there may be other variables at play in terms of what might actually be causing illness around the globe.
A Mechanistic Reason Why None of This Should Surprise Us
The idea that vaccination to generate antibodies in the blood stream has an effect on respiratory viruses has long been a controversial one. And as we've seen, it appears that the influenza vaccines never worked, which bolsters the argument that such antibodies fail to work at the right location—the mucosal membrane. This has been pointed out by Dr. Richard Urso, Dr. Ryan Cole, and others. Dr. Joseph Lee puts it thusly,
Never mind, I'll let you off the hook. No bet. The COVID antibody was barely present in 2020. The COVID antibody doesn't seem to have a path through the lung barrier into the lung alveolar cell area. The lung barrier can stop water molecules that are 18 Daltons in size and the COVID antibody is a gargantuan 145,000 Daltons in size. The lung barrier can stop WATER molecules. This barrier MUST be passed by the COVID antibody in order to reach the lung alveolar cells. But, this barrier WILL stop the COVID antibody.
We are not yet done. More to come…